
Stop! In the name of health—lessening low-value care

MacColl engages teams to ‘de-implement’ needless tests and treatments, doing less overused low-value care that might harm patients
For Michael Parchman, MD, MPH, it’s personal: “This is the first opportunity I’ve had to address a concern that has nagged at me for years: My profession’s central tenet is ‘first, do no harm.’ But in my career I know I’ve done unnecessary things that have harmed my patients, like overusing prostate-specific antigen (PSA) tests, although they seemed like the right thing to do at the time. Now I have a chance to do something about it.”
Taking action on overuse
That chance is a project called Taking Action on Overuse. Aiming to reduce unneeded tests and treatments, or “low-value care,” it is funded by the Robert Wood Johnson Foundation (RWJF) and directed by Dr. Parchman and Brian Austin. Dr. Parchman is the director of the MacColl Center for Health Care Innovation and a senior investigator at Group Health Research Institute (GHRI), and Mr. Austin is the associate director of the MacColl Center.
 |
|
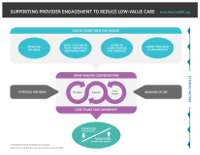
Supporting Provider Engagement |
Taking Action on Overuse recently produced an action planning framework to serve as a guide for supporting clinicians in reducing use of (“de-implementing”) tests and treatments that have proven to do more harm than good. Just one example: ordering X-ray images of the spine for first-time acute low back pain. The framework is based on a literature review and environmental scan—interviews with 23 leading U.S. health care organizations, including four site visits—with feedback from an advisory committee of diverse stakeholders including patients, clinicians, and health care leaders.
“We found that many health care organizations have nuggets of useful information on de-implementation that haven’t been shared widely,” says Diana Buist, PhD, MPH, a GHRI senior investigator who is also working on the project. “Our action planning framework and upcoming publications are a chance to do that.”
“Nationally, stakeholders see Group Health—our care-delivery system, health plan, foundation, and research institute alike—as thought leaders and exemplars in value-based care,” Mr. Austin says. “During our site visits, several people quoted Matt Handley back to us.” Matt Handley, MD, Group Health’s medical director for quality, has been working with Dr. Buist on the Group Health Foundation-funded Partnership for Innovation project to reduce low-value care, such as overuse of Pap tests, at Group Health.
Here and now
“This is a great historical moment to be taking action on overuse,” Mr. Austin says. “If we can do less of what might harm patients, we’ll be able to provide more patients with more of what helps them.” The United States must start giving people the care they need—no more, no less—because we have the world’s highest costs, without the best health outcomes, he adds. Part of the problem is care that is inappropriate and costly, including unnecessary testing that can lead to a “cascade” of more tests and treatments that may lead to patient harm.
“Choosing Wisely® has already established what tests and treatments are overused—and now our project is about how to do that,” Mr. Austin adds. The American Board of Internal Medicine (ABIM) Foundation and many medical specialty societies launched Choosing Wisely in 2012, partnering with Consumer Reports. More than 70 specialty society partners have listed recommendations for providers and patients to have conversations about tests and treatments that may be unnecessary and even harmful.
Thanks to Choosing Wisely, many clinicians and health systems agree that they need to stop providing care that evidence doesn’t support, Dr. Parchman says. But just like patients’ health behaviors, clinicians’ practice habits can be difficult to change.
“Clinicians are used to doing more and more, and that’s challenging enough,” Dr. Parchman says. “But it can be even more difficult to stop doing what you’re used to doing.” Especially in cases without obvious replacement services, it’s hard to explain to patients why doing nothing may be the best path.
“Everyone’s improvising on de-implementation now,” Dr. Parchman adds. “We all need a resource to show us how best to do this work.”
The Taking Action on Overuse framework is meant to be a roadmap for this uncharted territory. Instead of imposing solutions on clinicians—like abruptly deleting an option from the electronic health record—the framework recommends engaging them so they take ownership of stopping overused tests and treatments, which may or may not be included in Choosing Wisely.
The core of the framework is conversations between patients and providers on the potential for harm and among providers and care teams about how often a test or treatment is ordered. To create the conditions for productive conversations, the framework advises making this work a priority; building a culture of trust, innovation, and improvement; establishing a shared purpose and language; and committing resources to continuingly measuring use. In addition to measurement data, patient stories are the key to changing minds.
Next steps
Phase 2 of the project is ramping up now. For two years, the Taking Action on Overuse team will support and study use of the framework in three geographically diverse settings, yet to be chosen:
- An outpatient/ambulatory care setting.
- An acute inpatient care setting.
- Regional health care improvement collaborative.
Based on experience in these settings, the team will further refine the framework—setting the stage for then spreading it more broadly. RWJF grant 72546 supports this project. Others on the team include GHRI’s Paula Blasi, MPH; Diana Charbonneau, MA; Gabrielle Gundersen, MPH; Nora Henrikson, PhD; Leslie Jauregui; Lorella Palazzo, PhD; Robert Penfold, PhD; and Nicole Van Borkulo, MEd.
“Taking Action on Overuse is an exciting stretch for us at MacColl,” Mr. Austin says. “The hospital will be a new environment for most of us to work in. And we’re accustomed to tackling underuse of proven practices, rather than overuse of disproven ones. But like too little health care, too much can also harm people’s health. So this is important work.”
by Rebecca Hughes

co-researchers
Nora Henrikson, PhD, MPH
Associate Investigator
Paula R. Blasi, MPH
Senior Collaborative Scientist
Robert Penfold, PhD
Senior Investigator
Lorella Palazzo, PhD
Senior Collaborative Scientist


